In short
Dental keywords are some of the most expensive clicks in paid search — a single click on "dental implants near me" or "emergency dentist" routinely costs more than clicks in banking or real estate. At that price, every no-show and every unanswered message is not a minor inconvenience. It is a specific dollar amount walking out the door.

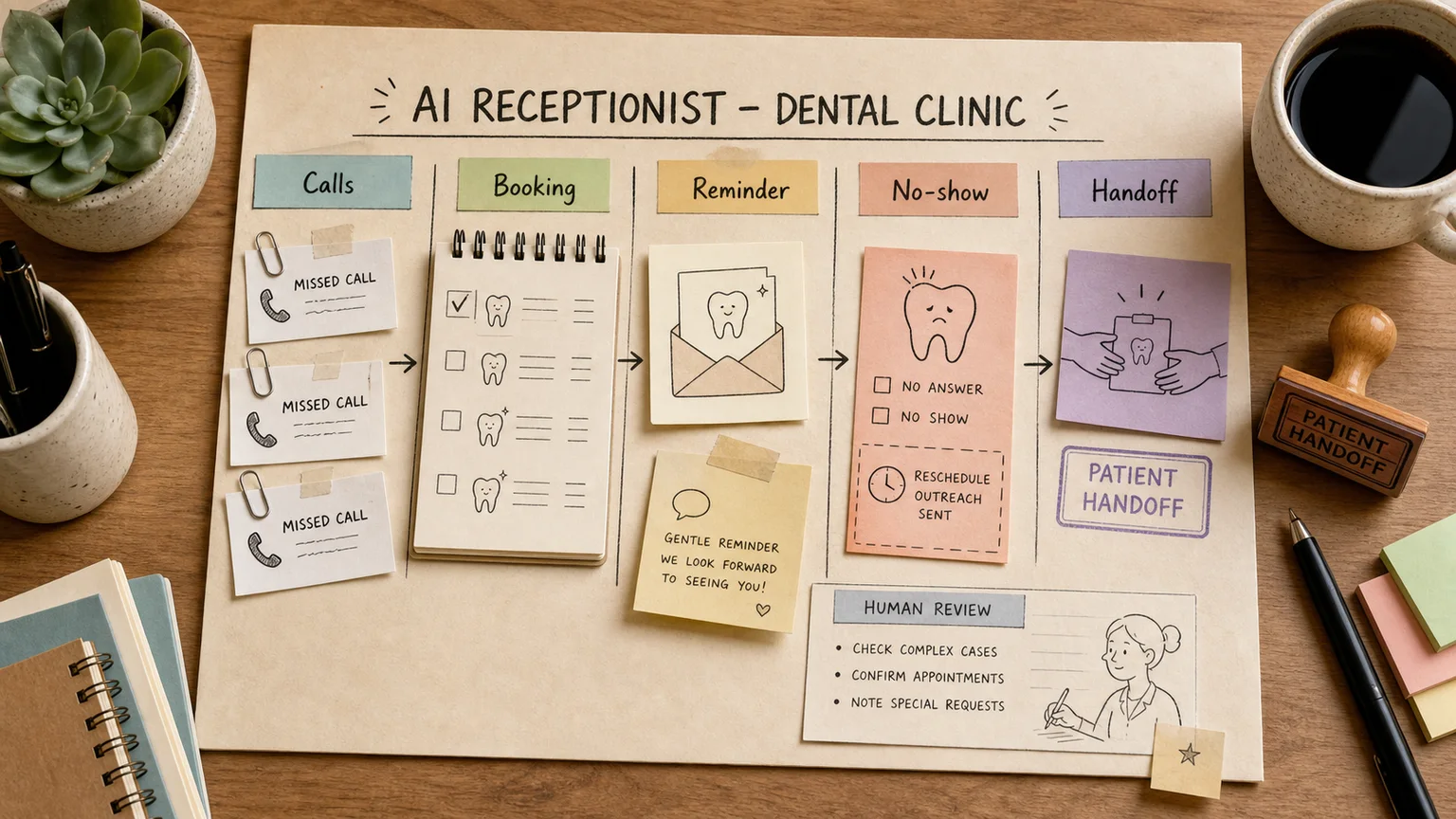
An AI receptionist for a dental practice is not a fancier phone tree. It is a layer that sits on top of the practice management system (Dentrix, Open Dental, Eaglesoft, or a newer cloud platform), answers the channels patients actually use, and does three unglamorous things well: gets people booked, reminds them so they show up, and brings back patients who are overdue for a cleaning or a follow-up. Here is how that actually gets built, and what should stay with a human.
Why a $200 no-show changes the math
A generic answering service treats every missed call the same way. A dental practice cannot afford to think that way, because the cost of a missed new-patient call and the cost of a missed hygiene recall are both real money, just in different ways.

Industry estimates put the average no-show cost per missed appointment at roughly $150 to $200 once chair time, prep, and lost same-day fill-in are counted. Typical no-show rates without active reminder management run 15 to 25 percent. For a practice booking a hundred visits a week, that is thousands of dollars a month evaporating on empty chairs — not because patients are careless, but because a single text reminder sent 48 hours out is easy to ignore and a single missed callback is easy to forget.
The second cost driver is response time on new patient inquiries. Someone searching "dentist near me" at 8 p.m. after a bad day is comparing three practices in the same ten minutes. Whoever answers first — even with a same-day slot proposal instead of a live person — usually gets the booking. A message that sits unread until the front desk opens at 8 a.m. has already lost that patient to a competitor down the street.
What the AI receptionist should actually do
The role is not to replace the front desk. It is to handle the repetitive first layer so staff spend their time on patients who are already in the building and on the judgment calls a bot should never make. The safety boundaries look a lot like AI for clinic reception in general medical practice — logistics yes, clinical interpretation no — but dentistry adds its own wrinkle: booking depends on matching a specific provider, procedure type, and sometimes treatment-plan stage, and the cost of getting that match wrong is a wasted chair slot.

Intake and initial booking
A patient texts, chats on the website, or calls after hours. The agent asks what they need (cleaning, new patient exam, pain, cosmetic consult), which provider or location they prefer, and what times work. If it has read access to the schedule, it proposes real open slots instead of a vague "sometime next week." Early on, it is safer to have the agent draft the booking for staff to confirm rather than let it write directly into the schedule.
Reminders and confirmation
A reminder two to three days out, a second one the day before, and a phone call if there is no response to either text — that sequence is what actually moves the needle on no-shows, more than any single channel alone. If a patient wants to reschedule, the agent should offer the next open slots with the same provider immediately, not just log "wants to reschedule" for someone to deal with later.
Recall and reactivation
Every dental practice has a list of patients who are six, twelve, or eighteen months overdue for a cleaning or a periodic exam. That list usually sits untouched in the practice management system because nobody has time to call two hundred people. An agent can work that list monthly, send a personal-feeling reminder, and offer a slot. Reactivating an existing patient costs a fraction of acquiring a new one through paid search, which is exactly why this workflow pays for itself faster than most marketing spend.
Pricing and prep questions
Cost of an implant, what to bring to a first visit, whether a filling hurts, how long a root canal takes — these are the questions every front desk answers ten times a day. A RAG-backed assistant can answer from the practice's own approved fee schedule and prep instructions instead of general knowledge about dentistry, which matters because a model that improvises a price the practice stopped offering six months ago creates a real billing headache.
Handoff to staff
A patient in pain, a billing dispute, a question about a warranty on prior work, anything that needs a clinical judgment call — the agent should not try to resolve it. It should collect context (who the patient is, what procedure, when, what they are describing) and hand the conversation to a staff member with a clean summary instead of a raw chat log.
Practice management systems and multi-location groups
A single-location practice usually does fine layering an AI agent on top of whatever it already runs — Dentrix, Open Dental, NexHealth, Weave, or similar. The agent reads the schedule and patient status through the platform's API and writes back only after staff confirm.
A group with five, ten, or more locations usually outgrows what a single practice management tool handles well. At that scale it is common to run a dedicated CRM layer across locations — tracking provider schedules, patient history, and per-location reporting in one place — with the AI agent as one more channel alongside phone calls and front-desk visits, not a bolt-on chatbot. The integration order that works in practice: start with read access to schedules and services, then let the agent propose slots, then let it book with staff confirmation, and only later allow unsupervised booking for low-risk visit types like a routine cleaning.
What should never go to the model
The agent never gives clinical advice. Symptoms, pain, treatment questions, and anything touching a diagnosis go to clinical staff, full stop. It does not reassure a patient in pain instead of getting them to a person who can actually help.
Prices and promotions come only from an approved, current fee schedule, not from the model's general sense of what dental work costs. Discounts and warranty claims follow written practice policy, not improvisation.
Patient records and protected health information need the same discipline as any clinical system: role-based access, logged actions, and no casual exports. In the US, that means designing around HIPAA from day one, not bolting it on after the pilot works. Before anything reaches live patients, run the mixed-language and edge-case messages — a garbled voicemail transcript, a one-word reply, a patient describing pain instead of asking about scheduling — through evals for AI projects rather than trusting a clean demo.
Running a 30-day pilot
Week one is not a vendor demo. Pull the last month of real patient messages, missed calls, and reschedule requests. See where time actually gets lost instead of guessing.
Week two, the agent runs as a copilot: it drafts replies, prepares booking suggestions, and stages reminders for staff to approve. No patient talks to the bot directly yet.
Week three, turn it loose on one narrow slice — reminders and confirmations for a single location, or recall outreach for patients overdue by six months. A narrow scope is easier to monitor and faster to fix if something goes wrong.
Week four, compare no-show rate before and after, response time on inbound messages, how many inquiries actually converted to a booked visit, and how many recall patients came back. If staff keep rewriting half of what the agent drafts, fix the workflow before expanding it.
This kind of build — multiple channels, a practice management system or CRM, reminders, and a clean handoff — is usually worth structuring as a proper AI agent rather than a standalone chatbot widget, because it needs memory of the location and provider, schedule access, and clear escalation rules.
What to measure
Beyond the no-show rate and response time, track two things separately: how many message-based inquiries actually turned into a booked and completed visit, and how often staff override or rewrite a slot the agent proposed. That second number is the most honest signal of whether the agent actually understands the practice's scheduling logic yet.
FAQ
Can a dental practice run booking entirely through text messages?
For a single provider with a light schedule, that works for a while. Once daily bookings climb into double digits or a second location opens, texts on a personal phone stop being a system and start being a place where requests quietly disappear. At that point the practice needs a shared system where booking status and patient history are visible to everyone handling that patient.
Does an AI receptionist replace front-desk staff?
No. It absorbs the repetitive first layer — answering, confirming, reminding, reactivating — so staff spend their time on people who are already in the chair and on decisions that need a person: clinical judgment, billing disputes, and anything that touches a patient's care.
What if the practice already uses Dentrix or Open Dental?
Don't migrate systems just to add AI. Connect the agent on top of what's already running: read access to the schedule first, reminders next, then slot proposals. Switching practice management platforms is a separate decision from adding an AI layer.
How fast does this pay for itself given expensive dental ads?
Usually faster than practices expect. Cutting the no-show rate by even a few percentage points recovers the cost of a pilot within one or two months, precisely because each saved appointment is worth more here than in almost any other local service category.
If missed messages or no-shows are already a known pain point, start with one narrow workflow — reminders for one location, or recall outreach for one overdue patient segment — rather than automating the whole front desk at once. Expanding from a working pilot is far easier than untangling a broad rollout that broke in week one.